
careQ: Digital Waiting Room Queue
Patients at a primary care office aren't just waiting, they are stuck in this liminal space that breeds frustration. To fix that, we gave them back their time. I served as the design and project lead for careQ, a service that visualizes the doctor’s office queue in real-time.
Overview
By mapping the friction between patient anxiety and staff workflow interruptions, we identified that the waiting problem was actually an information architecture problem that led us to prioritize system transparency over spatial redesign. What began as a challenge to improve the physical comfort of a waiting room quickly shifted when our research revealed that no amount of amenities could solve for the anxiety of the unknown. We didn't just redesign a room; we redesigned the relationship between patients and their care providers.
Project Reframe
Duration: 8 weeks for Service Design Class
Collaborators: Alice Qiu, Katres Brahmnhatt & Parker Gillis
Role: UX Design, Service Strategy, Project Management, Research
Tools: Figma, Miro, Canva
Audience
careQ was designed for two interconnected users: primary care patients and front desk receptionists. Patients were our primary focus, but it quickly became clear that their anxiety didn't stay in the waiting room. It directly disrupted staff workflow and even colored the care interaction before a doctor ever walked in. Solving for one without the other would have addressed the symptom, not the system.
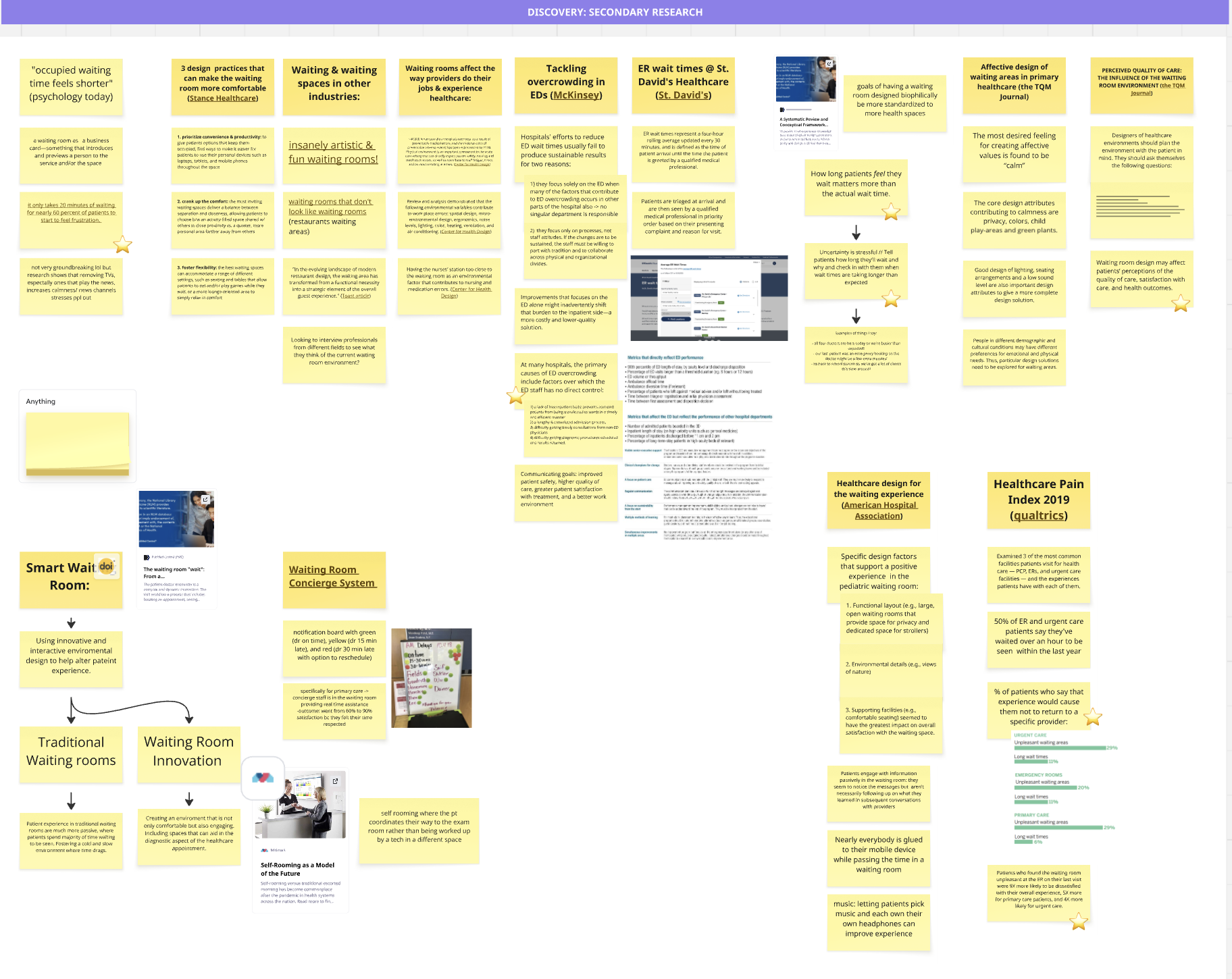
Foundational Research
To understand the waiting room as a system, we looked beyond the patient's chair. In two weeks we conducted targeted interviews and shadowed at a local clinic, realizing that any intervention for the patient would directly impact the receptionist's workflow. Because of our tight timeframe, we leaned heavily into secondary research on the psychology of waiting and found that patient frustration spikes at a 20-minute threshold regardless of physical amenities. The stress wasn't about the room's comfort. It was about the perceived loss of time.

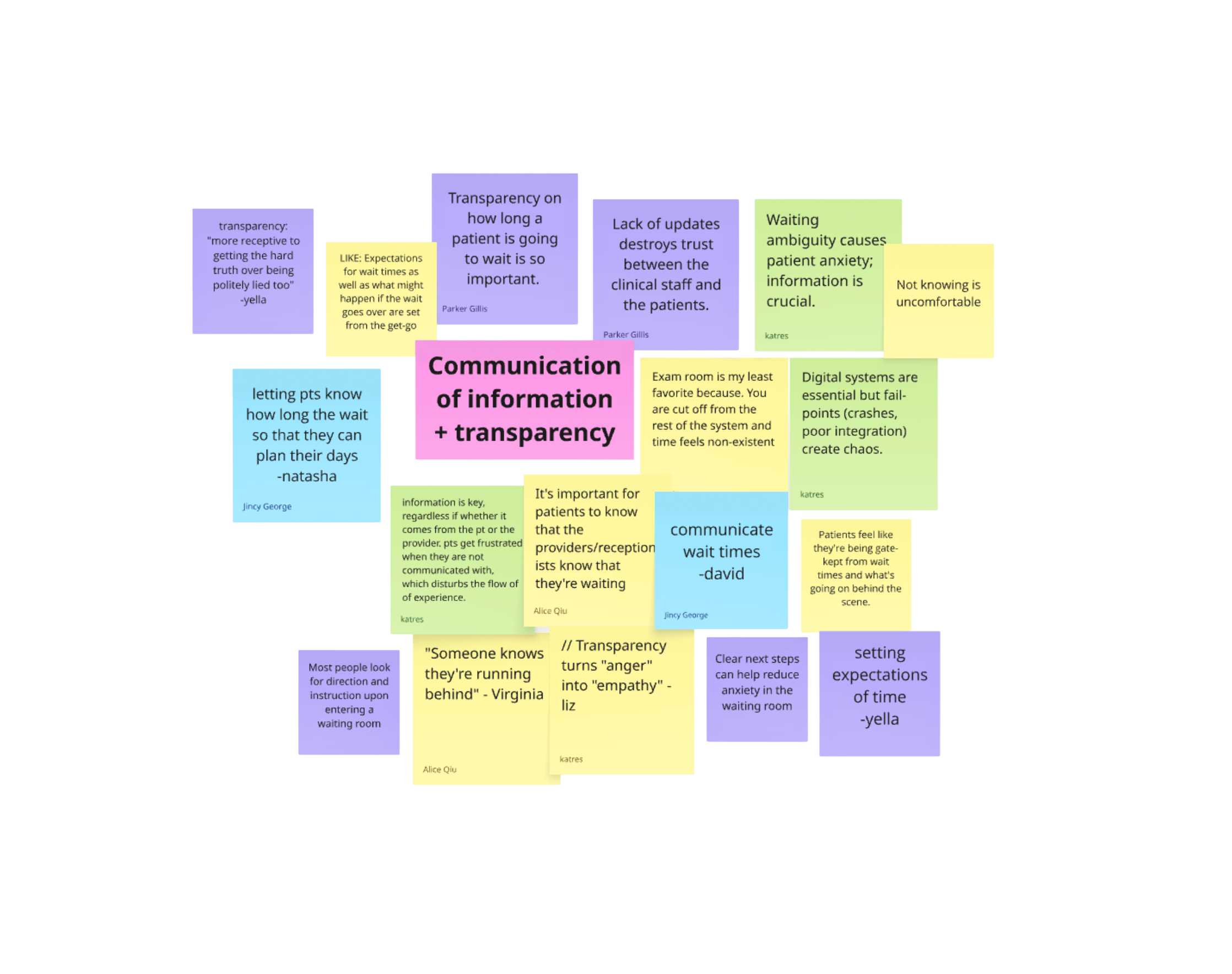
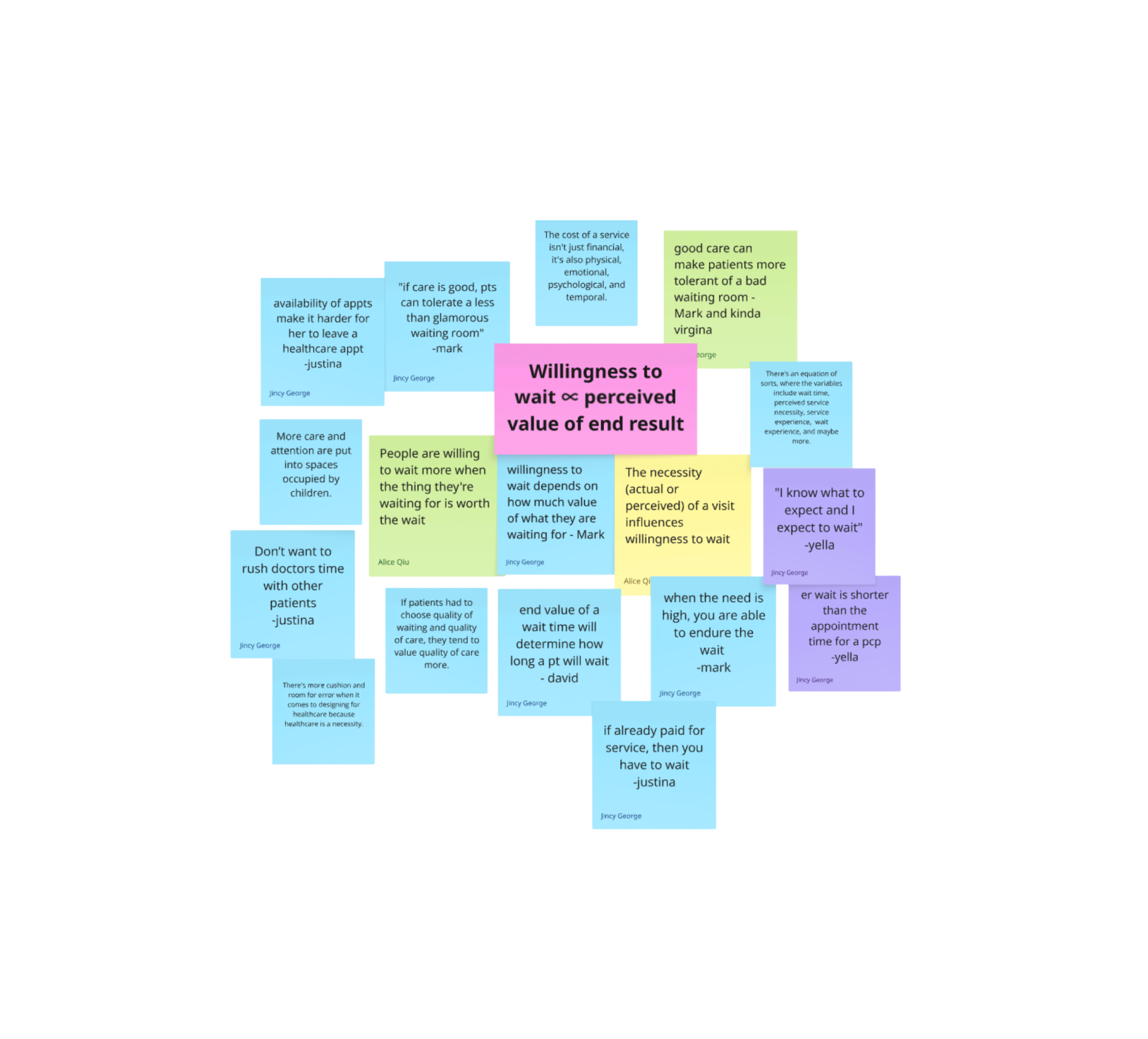
Insight Framework
Synthesizing our research revealed that for patients, waiting is not a passive act. It is an evaluation of respect. Our synthesis surfaced three core pillars that redefined our strategy and confirmed that our solution needed to be an expectation-management tool, not just a digital sign. By solving for transparency, we weren't just fixing a space, we were protecting the doctor-patient relationship before it even began

"Regardless of how long you tell me it’s going to be, I’m stuck with this (health) service no matter what. I prefer to know how quickly to be in and out, but with the visual system so you can mange your time better”.
-31 year old female patient
Ideation & Prototyping

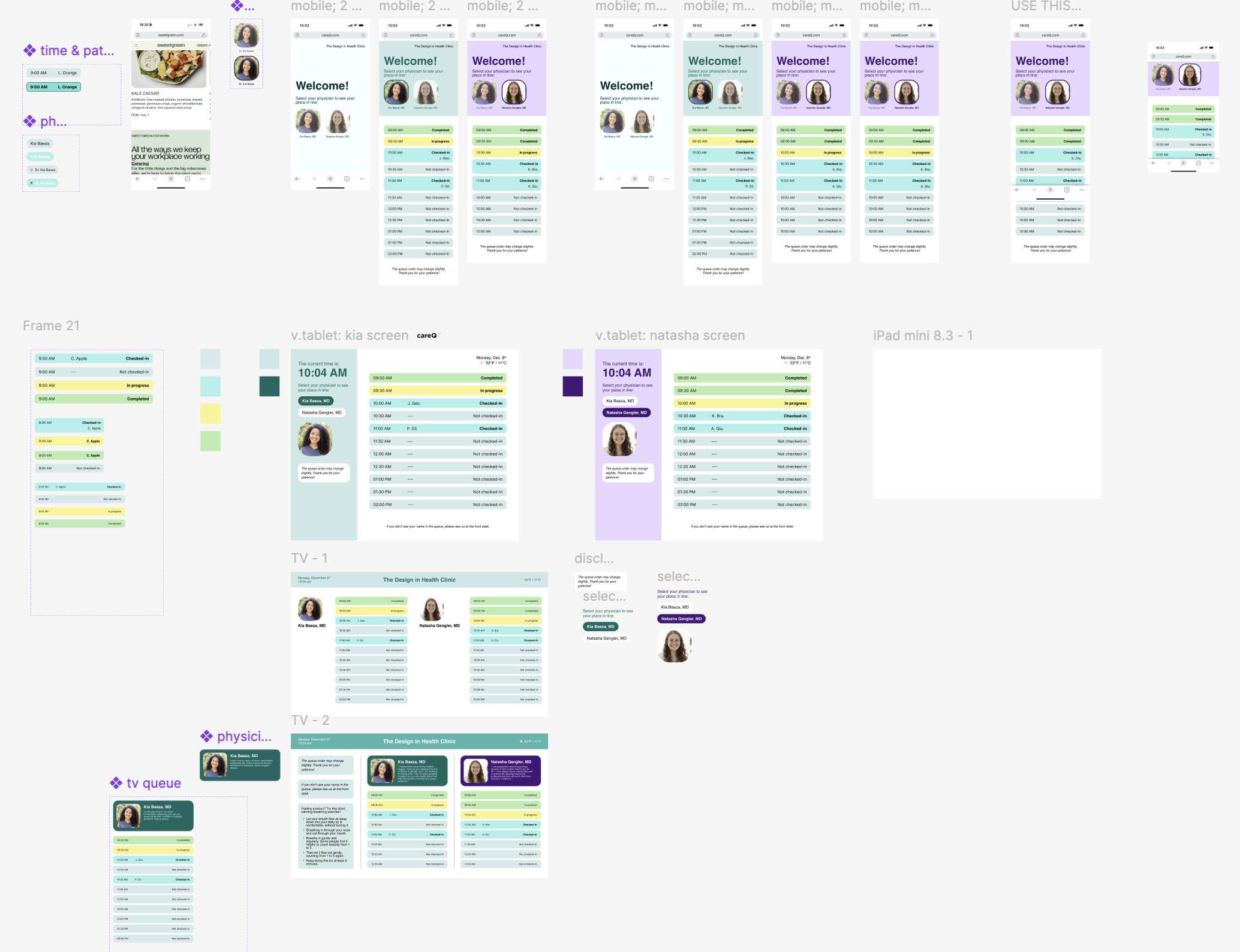
Our brainstorm surfaced 50+ ideas across three directions: environmental improvements, digital distraction tools, and transparency-based solutions. Early user feedback quickly eliminated the first two. Patients didn't want entertainment, they wanted acknowledgment. From there I led the team in building a decision framework grounded in our research insights and a clear set of design guardrails, allowing us to cut popular ideas like tablet consoles that felt intuitive but didn't serve our core goal.
Design Guardrails:
Core Requirements: Real-time updates, accessible across TV and mobile, HIPAA-compliant, and integrated into existing staff workflow without adding burden.
Strategic Exclusions: We avoided features that felt like distractions and precise wait times, as our research showed these inadvertently signaled a long wait and increased frustration.

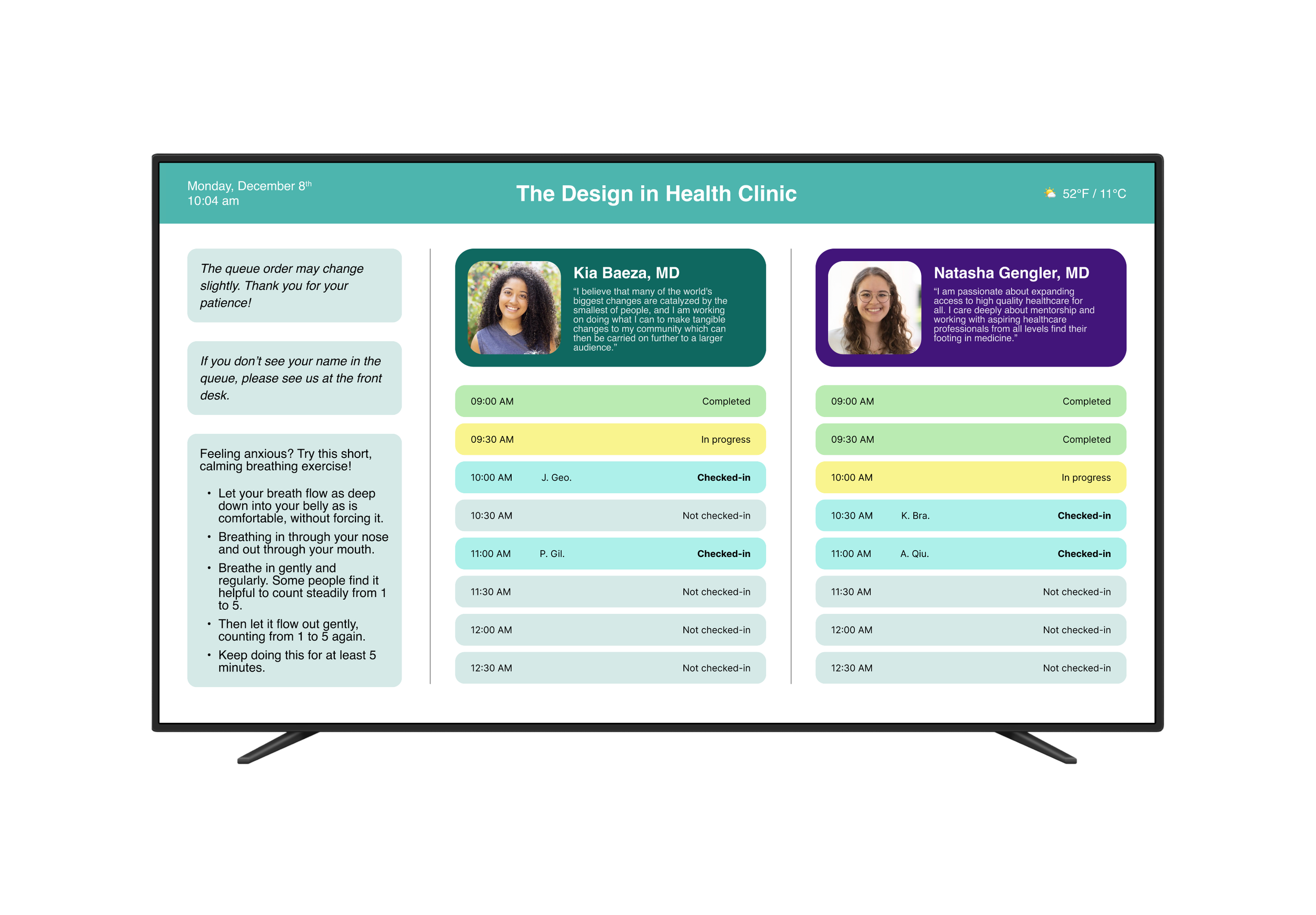
Final Outcome

The result was careQ: a dual-touchpoint service replacing waiting room uncertainty with real-time transparency. Upon check-in, patients see their HIPAA-compliant name in the queue and monitor their progress via a wall-mounted lobby display or their own mobile device. Beyond the UI, we delivered a multi-phase implementation plan including a 30-day pilot program and staff walkthrough, ensuring the transition was supported by internal IT and front-desk workflows.

The Impact: We moved from a goal of decorating a room to redesigning a relationship. The concept received positive feedback from instructors and peers, validating that transparency-first addressed a real and recognizable problem in healthcare.
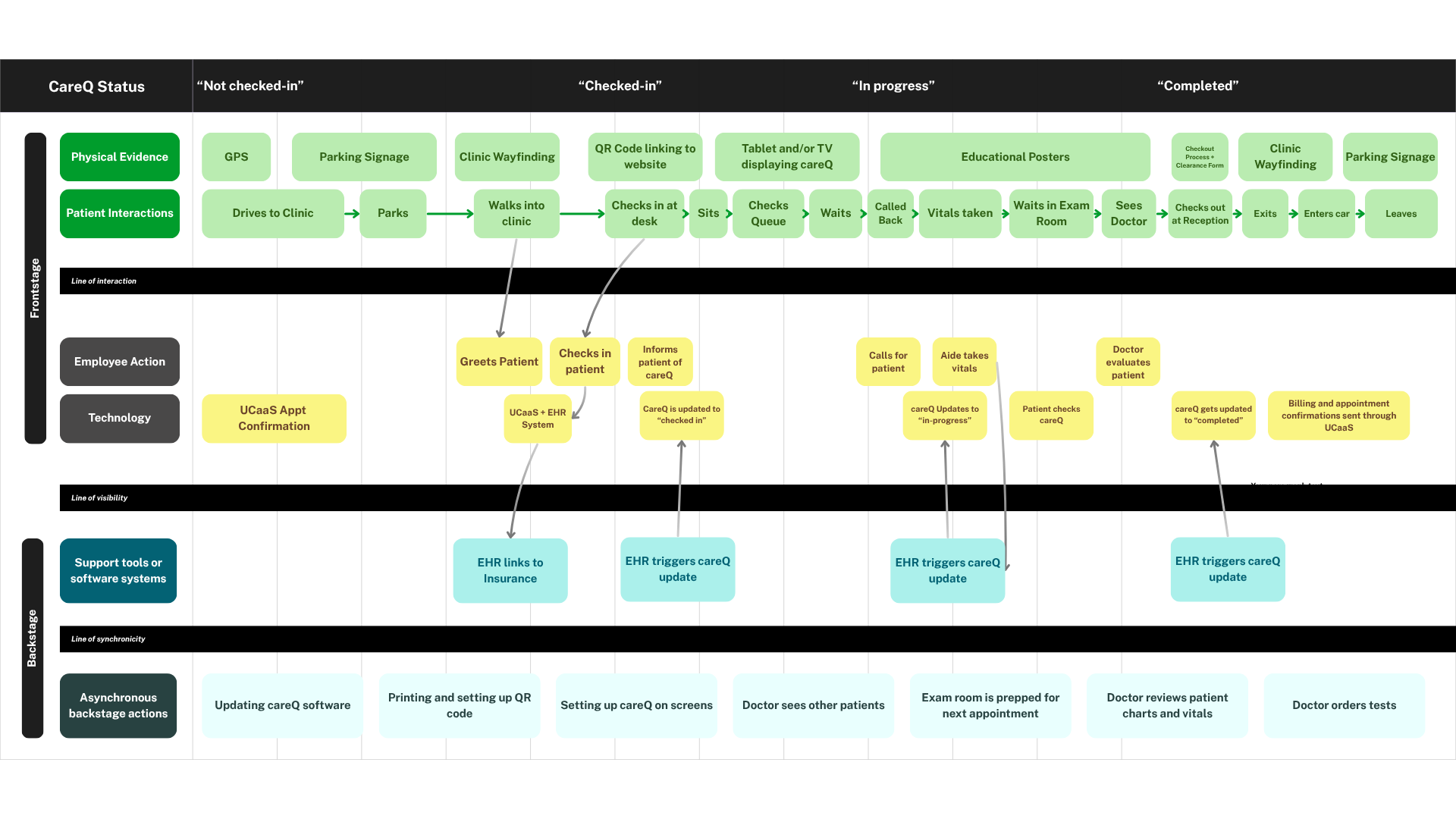
While the UI focused on transparency, the Service Blueprint was where we solved for feasibility. I led its development to map the Line of Visibility from my emergency room experience, ensuring real-time patient updates were triggered by simple low-friction staff actions. A receptionist changing a status to “Arrived” would automatically update the careQ queue, keeping the back-stage invisible to patients while making the front-stage predictable.
Retrospective
Solving the Right Problem
The waiting room problem wasn't about physical comfort. It was about a lack of agency. Shifting from spatial design to wait-time transparency meant addressing the root cause rather than decorating around it.
The Blueprint as a Diagnostic Tool
If I were to approach this project again, I would lead with a service blueprint immediately after research. Using it earlier would have surfaced systemic friction points like the Acknowledgment Gap before we began ideating, streamlining our path to the final solution.
Failing Fast and Design Guardrails
When initial concepts for kiosks and tablets failed to resonate with users, we pivoted rather than doubled down. The Design Guardrails became essential. By stripping away distractions and focusing on functional transparency, we proved that in healthcare, less is more.